Esophageal adenocarcinoma is the fastest growing cancer in the United States. In total, it affects about 1.5 million people per year worldwide and 38,000 in the US alone. There has been a 6-fold increase in the last 3 decades, accounting for 60% of esophageal cancers. This is one puppy you don’t want to mess with; don’t even get me started on colorectal cancer!
Gastroenterology accounts for 10% of the PANCE, so make sure you pay attention during this part of your didactic phase! Knowing that, you had better take a step into gastroenterology with your thinking cap on ready to learn about new disease and therapy that can affect the way you provide care everyday.
Most Commons in Gastroenterology
- Heartburn (pyrosis) - most common symptom of esophageal disease
- GERD (Gastroesophageal reflux disease) - most common disorder of the esophagus
- Ulcerative Colitis - most commonly affects young adults in 2nd and 3rd decade of life, but 2nd peak in 7th decade
- Most common in N. America, England, N. Europe, and Australia
- More common in industrialized countries
- More common in higher socioeconomic status
- Important: Ulcerative colitis increases the risk of colorectal cancer
- Crohn’s Disease - most common between 15-30 years of age, though can present at any age
- More common in industrialized countries
- More common in higher economic status
- Most common in N. America, England, N. Europe, and Australia
- Skip areas common: The most common distribution pattern of Crohn’s disease is ileocecal, which involves the distal portion of the small intestine (terminal ileum) and the proximal large bowel (40% of patients)
- Most common skin lesions in IBD: pyoderma gangrenosum and erythema nodosum
- Esophageal cancer - most common in men
- Most common in African Americans (5 times increase in incidence)
- Incidence increases after age 40 with each subsequent decade
- SCC Risk Factors - most commonly alcohol consumption and smoking
- Adenocarcinoma - most common in caucasian men
- Primary risk factor: Barrett’s esophagus
- Most adenocarcinomas (90%) develop in the distal esophagus
- Most common symptom of esophageal carcinoma: dysphagia
- Constipation - most common in women
- Most common causes of constipation: inadequate fiber or fluid intake and poor bowel habits
- Most common cause of CRAP (chronic recurrent abdominal pain) in children
- Primary (functional) Constipation) - more common than secondary
- Diarrhea - common cause of death in developing countries (WHO)
- Second most common cause of infant deaths worldwide due to dehydration and electrolyte deficiencies
- Acute Diarrhea (<2 weeks) - most commonly caused by infectious agents, bacterial toxins (preformed or produced in the gut), or medications.
- Most common viral agents: Rotavirus and Norovirus (Norwalk)
- ETEC (Enterotoxigenic E. coli) - most common cause of Traveler’s diarrhea
- EHEC (Enterohemorrhagic E. coli) - most commonly acquired from contaminated meat
- Campylobacter jejuni - most common type of acute bacterial diarrhea in US
- Giardia lamblia - most common intestinal protozoan in US
- Most important risk factor for Traveler’s diarrhea is the geographic destination
- South Asia = very high risk
- Lowest risk = Europe, North America (excluding Mexico), Australasia, Northeast Asia
- Celiac Disease - most common in women of European ancestry
- Most common causes of Osmotic Diarrhea: carbohydrate malabsorption (lactose, fructose, sorbitol), laxative abuse, and malabsorption syndromes
- Irritable Bowel Syndrome - most common cause of chronic diarrhea in young adults
- Pathogens most commonly involved with diarrhea
- Protozoans: Giardia, E. histolytica, Cyclospora
- Intestinal nematodes
- Bacteria: C. difficile, Aeromonas, Plesiomonas
- Immunocompromised hosts: Cryptosporidium, CMV, MAC
- Most common causes of Chronic Diarrhea: medications, IBS, lactose intolerance
- Acute Pancreatitis - the most common causes are gallstones (45%) and alcohol (35%)
- Chronic Pancreatitis - the most common nonobstructive cause is chronic alcoholism (70%)
- Pancreatic Adenocarcinoma - “painless jaundice” associated with cigarette smoking and high mortality rate
- Irritable Bowel Syndrome - one of the most common GI conditions (25-50% of GI clinic referrals)
- 10-15% of US population has IBS
- Occurs in any age - more common in younger patients, mostly women
- Diverticulosis - presence of diverticula
- Common in Western countries (western diet, lifestyle)
- Prevalence increases with age (60 - 60%); most common cause of lower GI bleed in elderly
- Most commonly found in the sigmoid colon (western countries) or right colon (Asia)
- Most common colonic source of severe hematochezia
- Diverticula - most common cause of lower GI bleeding (35% of cases)
- Do not confuse diverticulosis and diverticular bleeding with diverticulitis (infection and inflammation of the diverticula) which is not associated with LGI bleeding
- Paralytic Ileus - most commonly seen in hospitalized patients
- Small Bowel Obstruction - most common cause is adhesions after abdominal surgery
- Large Bowel Obstruction - most common cause is neoplasm (colon cancer)
- Acute Appendicitis - most common abdominal surgical emergency in the US
- Peptic Ulcer Disease - most common cause of upper GI bleeding
- 55% of all UGIB
- Gastric Cancer - one of the most common forms of cancer worldwide
- 870,000 new cases per year
- 650,000 deaths per year
- 60% occur in developing countries, highest incidence in East Asia, South America, and Eastern Europe (less common in US)
- Most common complication of decompensated alcoholic cirrhosis: Ascites
- Most common test performed to determine Hepatic Encephalopathy: ammonia
- Does not correlate with severity or diagnose HE
- Hepatitis B Virus (HBV) - most common in African Americans and Hispanics in US
- Also common among Alaskan Eskimos, Pacific Islanders, Africans and immigrants of countries with endemic infections and low socioeconomic groups
- Primary Hepatocellular Carcinoma (HCC) - one of the most common tumors in the world
- Most common in men; peaks in 50-60
- High association with cirrhosis, or if infected with HBV/HCV
- Fatty liver disease (NASH) increases the risk
- Tubular Adenomas - most common adenoma (CRC)
- Villous Adenomas - highest risk of cancer
- Indirect inguinal hernia - most common hernia
- Common in premature babies, and women > men
- Femoral Hernia - more common in multiparous women
- Indirect inguinal hernia - more common in women than femoral hernia
- Gallstone disease - most common gastrointestinal reason for hospitalization in the US
- 321,000 elective cholecystectomies (1996)
- Gallstones - 2X more common in women than men
- Prevalence increases after age 50+
- Cholesterol stones - most common type of stone
- Black pigmented stones - more common in patients with cirrhosis or chronic hemolysis
- Biliary colic - most common presenting symptom of cholelithiasis
Other Helpful Hints
- “Bird’s Beak” Esophagus - Achalasia on barium swallow
- Nutcracker esophagus - diffuse esophageal spasm
- Stovepipe esophagus - scleroderma of the esophagus (systemic sclerosis)
- “Rice Water Stool” - Vibrio cholera; abrupt onset grey, liquid diarrhea due to hypersecretion of water and chloride ion
- Difference between Ulcerative Colitis and Crohn’s Disease
- Crohn’s - small bowel involvement, skip lesions, pain
- Ulcerative Colitis - bloody diarrhea, involvement of the rectum and a continuous, superficial spread of the disease
- The “Football Sign” - you must scroll down on the page and hover to see the example. This is a wonderful website for radiology.
- Goodsall’s Rule - is applied to the examination of anal fistula. It states that:
- If the external opening of a fistula lies posterior to a line drawn from horizontally then it tracks around the anus laterally and opens into the midline posteriorly.
- If the external opening lies anterior to this line, then it opens directly into the anal canal
- Nissen Fundoplication - surgical treatment for GERD or hiatal hernia
- Important Gastric Cancer Signs (a few) - keep in mind these aren’t seen until the advanced disease state
- Sister Mary Joseph's Node (Periumbilical)
- Virchow’s Node (Supraclavicular)
- Krukenberg’s Tumor (enlarged ovary)
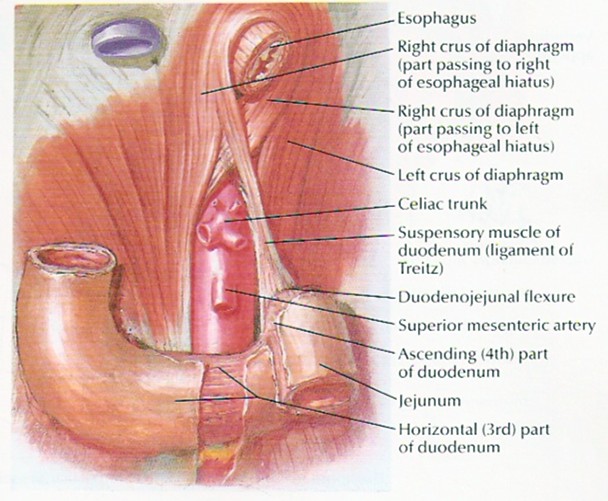
- Ligament of Treitz - tissue that connects the duodenum to the diaphragm
- Divides the GI tract into upper and lower portion
- Nasogastric (NG) Lavage - can help differentiate between UGIB and LGIB
- Blood Aspirate: confirms UGIB
- Saline: non-daignostic
- Bilious Aspirate: “negative” for UGIB
- Hematemesis - “coffee ground” emesis or bright red blood
- Hematochezia (BRBPR) - passage of bright red blood or maroon stools from the rectum that may or may not be mixed with stool
- Indicates LGI bleed
- Very brisk UGI bleed can present with hematochezia (>1000 mL blood)
- Laennec’s Cirrhosis - fatty liver, fibrosis, and nodularity in severe protein deficiency seen in children
- Also seen in alcoholics, hence alcoholic cirrhosis also referred to as Laennec’s
- Maddrey’s Discriminant Function and Composite Clinical Laboratory Index (CCLI) - both used to predict mortality of alcoholic liver disease patients. Nutritional status is the most predictive of prognosis.
- Child-Turcotte Pugh (CPT) Score and MELD Score - both predict mortality for hepatic cirrhosis patients. I recommend using the MELD score because it is also used by UNOS, which is the organization that determines who receives liver transplants.
- Cullen’s Sign (periumbilical ecchymosis) - Superficial edema and bruising in the subcutaneous fatty tissue around umbilicus; sign of intraabdominal bleeding; hemoperitoneum, pancreatitis, ectopic pregnancy;
- Grey Turner’s Sign (flank ecchymosis) - bruising of the flanks (between rib and hip); sign of hemoperitoneum
- Grey-TURNer’s sign is located when you TURN towards your flank
- CUllen’s sign is located around the Umbilicus
- Caput Medusa - recannulization of the umbilical vein
- Striae - weight gain, pregnancy or Cushing’s Syndrome, exogenous steroid use
- Rectus Diastasis - separation of the rectus abdominis into R and L; occurs in pregnant (post-partum) women and newborns
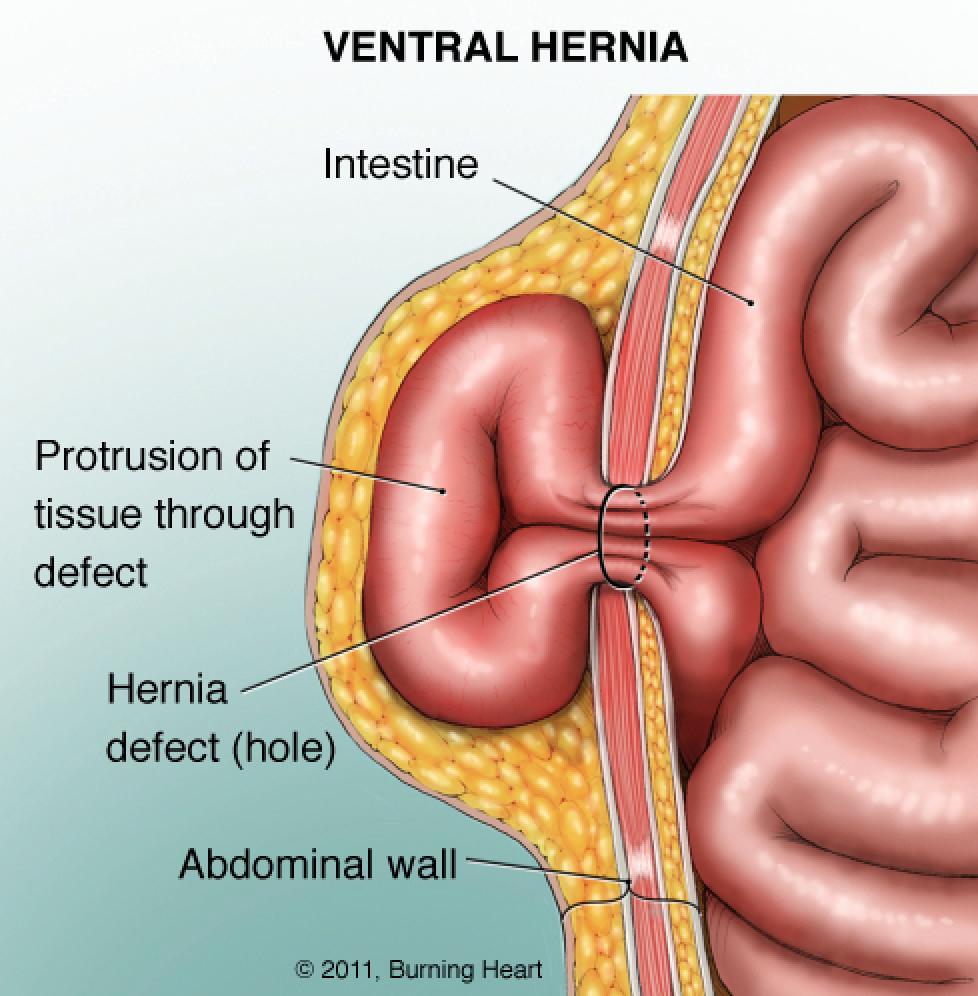
- Ventral Incisional Hernia - An incisional hernia is a type of hernia caused by an incompletely-healed surgical wound. Since median incisions in the abdomen are frequent for abdominal exploratory surgery, ventral incisional hernias are often also classified as ventral hernias due to their location. Not all Ventral Hernias are from incisions, as some may be caused by other trauma or congenital problems.
- Fluid Wave Test - In medicine, the fluid wave test or fluid thrill test is a test for ascites (free fluid in the abdominal cavity). It is performed by having the patient (or a colleague) push their hands down on the midline of the abdomen. The examiner then taps one flank, while feeling on the other flank for the tap. The pressure on the midline prevents vibrations through the abdominal wall while the fluid allows the tap to be felt on the other side. The result is considered positive if tap can be felt on the other side. However, even with the midline pressure, transmission through the skin must be excluded. A positive fluid wave test indicates that there is a free fluid (ascites) in the abdomen. When one side of the abdomen is pressed, the other side may also be painful due to the transfer of the fluid in it.
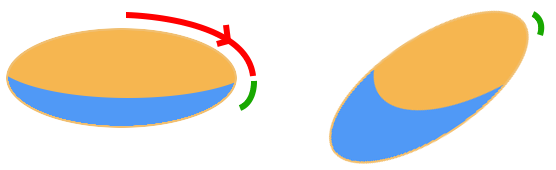
- Shifting Dullness - To perform the test, first the midline of the abdomen is percussed eliciting a resonant note due to gas in the abdomen. If there is no area of resonance then the test cannot be performed. Percussion is then moved progressively more lateral (away from the examiner) - this is depicted as the red section in the diagram on the right - until the note becomes dull, as depicted by the green section. The examiner's index finger remains on the resonant side, and the middle finger remains on the dull side, straddling the fluid-air level. The patient is then asked to lean on their right lateral side (assuming the examiner used the traditional right sided approach). This stabilises the patient by sandwiching them between the examiner's hands and body. It is imperative that the examiner's fingers stay in the same position. After waiting sufficient time for any fluid to shift (up to 30 seconds), the dull position is then percussed. It may now be resonant. The percussion may now be performed down the anterior side until a new dullness is found. To confirm a positive result it is recommended that the now resonant area become dull again when the patient is back in the supine position. If the borders between tympanic (resonant) and dull notes remain the same, the person probably does not have ascites, or has less than 2 litres of free fluid present. If the fluid causing the dullness was not free, then the air-fluid level would not move. Shifting dullness is usually present if the volume of ascitic fluid is greater than 1500 ml. If low volume ascites is suspected, then an attempt to elicit the puddle sign may be performed.
- Murphy’s Sign - inspiratory arrest during deep palpation of RUQ
- Hook fingers under right costal margin
- Ask patient to inspire deeply
- Sudden stop in inspiration constitutes (+) sign = cholecystitis
- Patient supine, place hand at 90 degrees and press deeply into abdomen with fingers away from area of discomfort
- Rapidly withdraw hand
- Will cause sharp, stabbing pain at site of peritoneal inflammation
- Rovsing’s Sign - deep palpation in the left lower quadrant produces pain in right lower quadrant (appendicitis); variation on rebound tenderness.
- Iliopsoas Muscle Test (Psoas Sign)
- Patient supine; place hand over R lower thigh
- Ask patient to raise leg, flexing at hip while you push down
- If (+), patient will have right lower quadrant pain (appendicitis)
- Additionally, you can perform the test by having the patient turn on their left side and extending their R leg
- Patient supine, have patient flex R leg at hip with knee to 90 degrees
- Grasp ankle & internally rotate at the hip
- Produces pain at the hypogastric region (RLQ)
- Used in suspected ruptured appendix or pelvic abscess
- McBurney’s Point Tenderness - indicative of appendicitis
- Palpating the Kidneys and CVA Tenderness
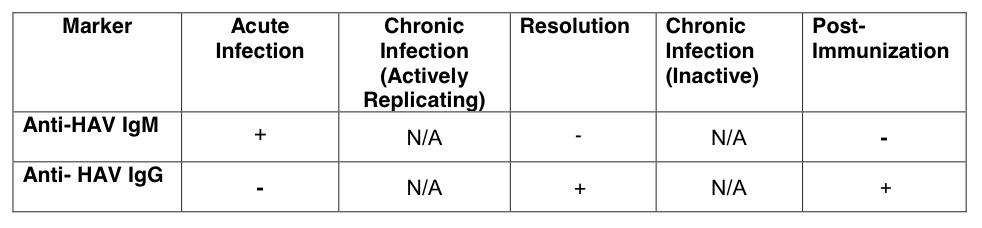
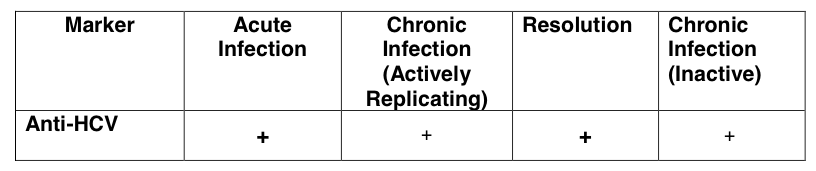
- Hepatitis Serologies
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Falling platelets - single most common laboratory abnormality seen and ignored or referred to hematology for work up (fibrosis progression)
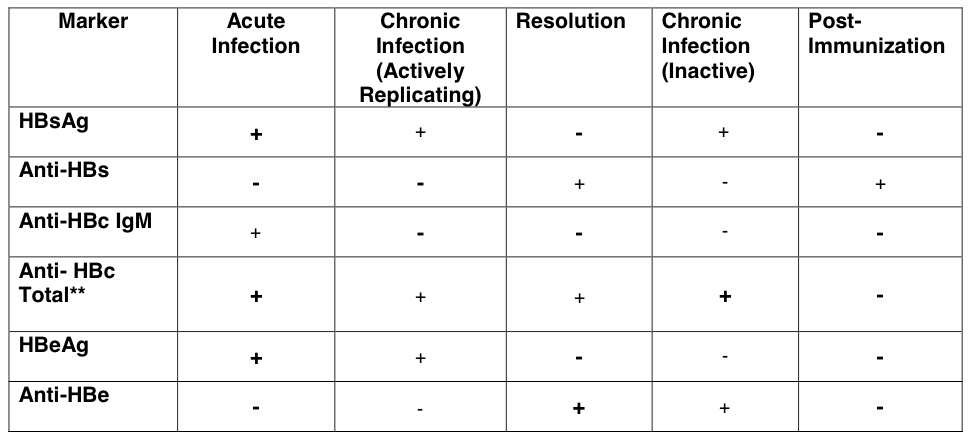
- If resolving infection
- HBeAg disappears, HBe Ab appears
- HBsAg disappears, HBs Ab appears
- How to distinguish if someone is vaccinated versus recovered? If they are vaccinated, they will have no positive Anti-HBc Total, and the only (+) serology will be HBsAb, while an immune/recovered patient will show positive HBc Total Ab (+) in addition to HBsAb and anti-HBe.
- AJCC (TNM) Staging System for Colon Cancer
- Important to note that for colon cancer, as opposed to other cancers, such as breast and pancreatic cancer, the “T” represents the extent of primary tumor invasion into the wall of the intestine and nearby structures (i.e. the depth of invasion through the bowel wall) and not the size of the tumor as in other cancers.
- If a patient has colon cancer, the most common site of metastasis is the LIVER, while if a patient has rectal cancer, the most common site of metastasis is the LUNG.
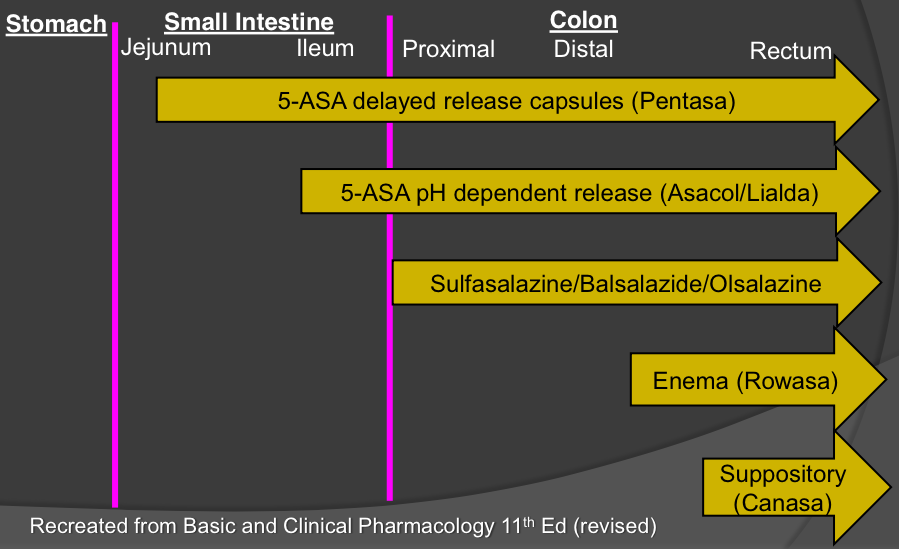
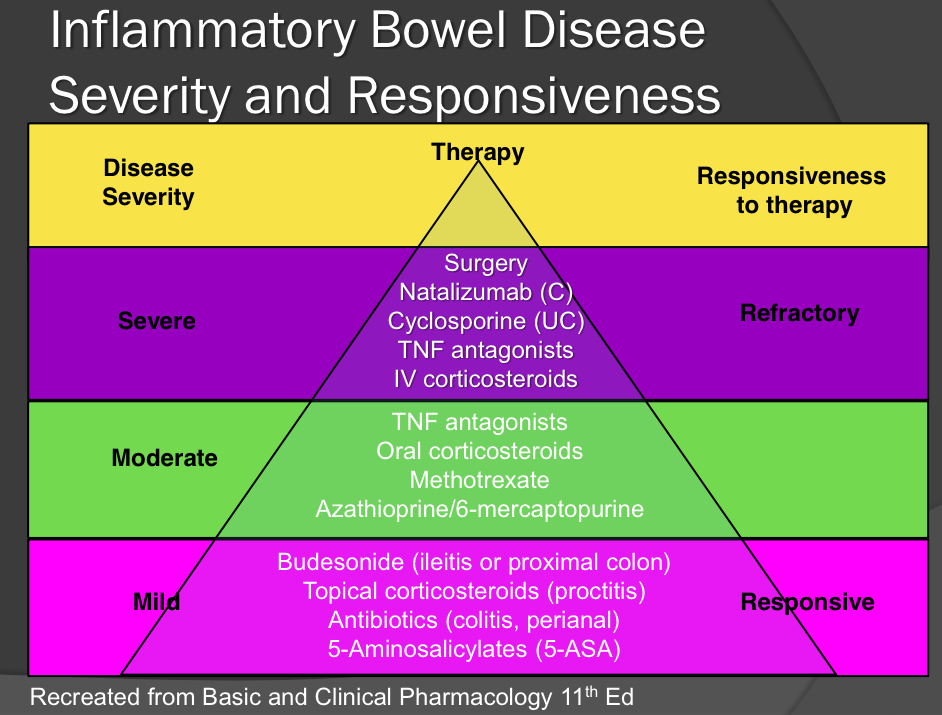
- Inflammatory Bowel Disease Therapy
Sources:
Current Medical Diagnosis and Treatment 2015
Cecil Essentials of Medicine, 8th edition
No comments:
Post a Comment
Leave a comment with feedback, questions, or inquiries for Paul. He will try to respond within 1-2 weeks.