Most Commons in HEENT for Physician Assistants
HEENT (EENT) makes up 9% of the PANCE and is one of the most common “bread and butter” medicine topics you’ll come across. Below is a combination of “most commons”, “buzzwords”, and other clinical pearls I have come across since completing my didactic year. I compiled this in order to help myself prepare for the PANCE and for rotations. I hope it helps you in your studies as well.
- Head
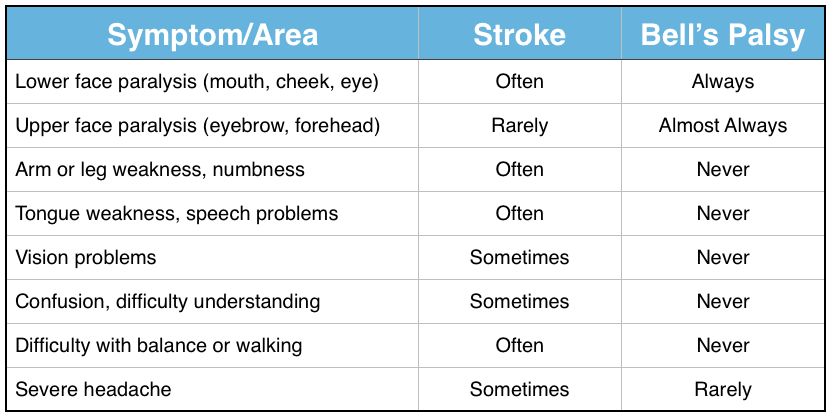
- Onset within 72 hours
- Loss of taste sensation in anterior ⅔ tongue (chorda tympani)
- Ears
Acute Otitis Media
 |
Otitis Externa - Bacterial
 |
Otitis Externa - Fungal
 |
MC: viral (45-70%), S. pneumo (25-50%), H. Flu (15-30%), M. Cat (20%)
MC (pediatric): S. pneumo
|
MC Path: Pseudomonas (50%), S. aureus/St. pneumo (40%), sterile (10%)
|
MC Path:
Aspergillus-niger (black), -flavus (yellow), or -fumigatus (gray)
Candida albicans (white)
|
Pain when supine or leaning forward, pulling on ear
Fever, hearing loss, aural fullness, pressure
PE: red TM, purulence, pre- or post-auricular LAD with cervical LAD, loss of cone of light
Associated rhinitis
Ruptured TM = drainage
Tuning fork: BC > AC
|
Pain with movement of pinna or eating
Conductive hearing loss
PE: swollen, red, yellow/green discharge, foul smelling, pre- or post-auricular LAD
+/- cellulitis of face
Tuning fork: BC > AC
|
ITCHY
Weeping, pain, hearing loss, aural fullness
PE: swollen, hyphae +/- spores, moist/wet-appearance |
TX: most resolve spontaneously
Mild: no ABX, reevaluate 2-3 d
Uncomplicated, previously untreated: HD (80-90 mg/kg/d) Amoxicillin or Augmentin x 10-14 d or IM ceftriaxone
Switch ABX 48-72 h if no resp.
PCN allergy: Sulfonamide + Erythromycin or Clindamycin, FQ
Do not use: antihistamines, decongestants
|
TX: hygiene, clean, otowick, topical analgesics
Otic drops: Ciprodex, Floxin
Contraindicated: irrigation or Gentamicin/Tobramycin with perforated TM
|
TX: hygiene, clean
Topical antifungal powder +
Antifungal otic drops: acetic acid, Vosol
Prophy: 1:1 ETOH/white vinegar in each ear after showering
Contraindicated: Lotrimin with perforated TM
|
Chronic Otitis Media (recurrent)
|
3+ AOM in 6 months OR
4+ AOM in 1 year
Autophony - can hear your echo
|
SX: continued pressure or fullness after resolution of infection, hearing loss, tinnitus, increased sensitivity to loud noises, not painful
PE: dull TM with decreased movement, hearing loss, speech delay
|
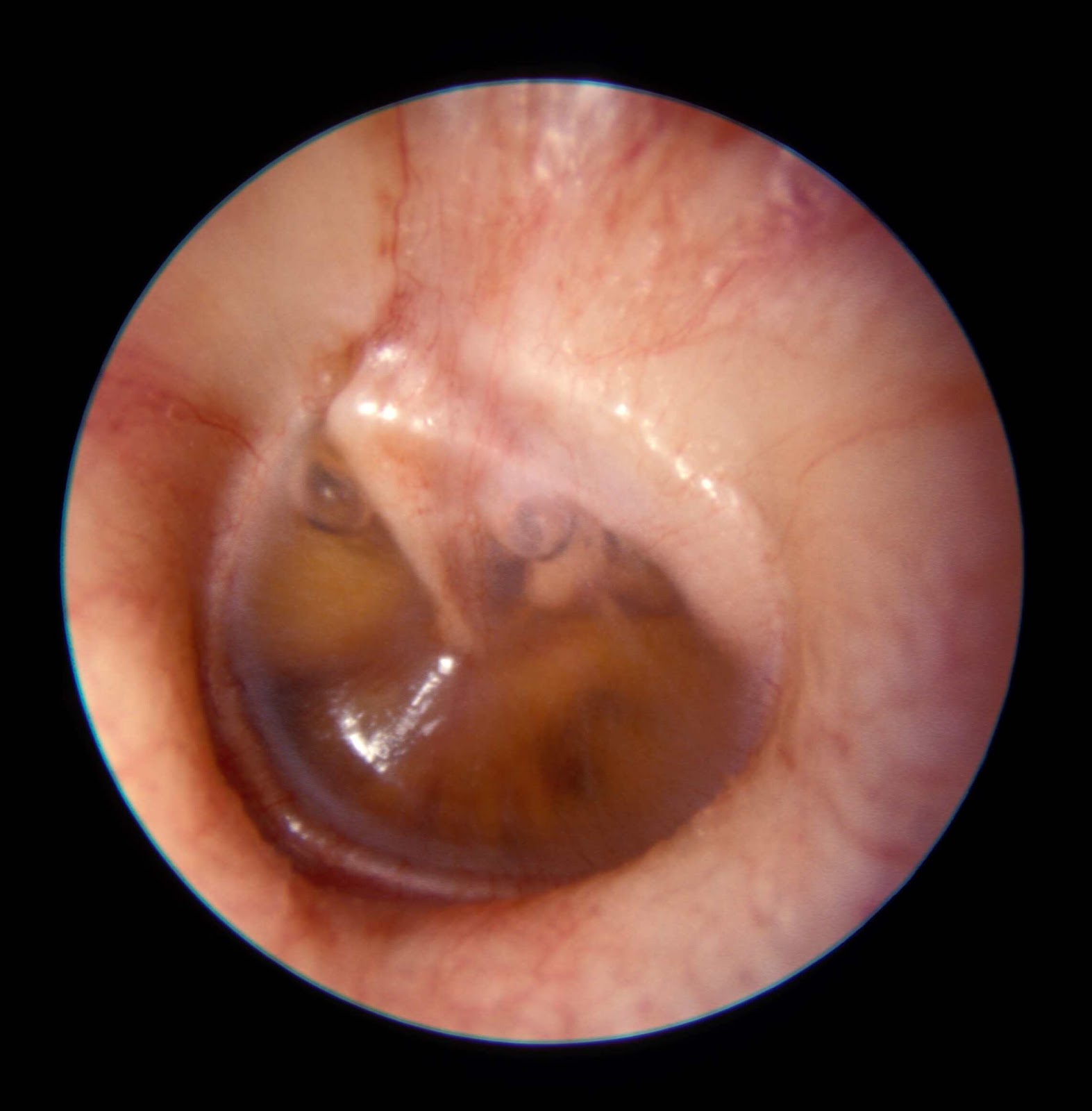
Serous Otitis Media
HX: recent viral URTI, sinus infection, flare of allergies, flying while congested, recent AOM, adenoid hypertrophy, nasopharyngeal mass
TX: resolves slowly (up to 12 weeks), follow up 4-6 W, nasal steroid sprays, short course of PO steroids
Do not use: antihistamines, decongestants
|
Fullness, hearing loss, pressure, popping/gurgling after a yawn or blowing nose, dizziness or swimming sensation
Unilateral or bilateral
PE: retracted TM, amber or “coca cola” colored fluid, displacement of cone of light, air bubbles behind TM, pneumatic otoscopy reveals decreased movement of TM
Tuning fork: BC > AC
|  |
Cholesteatoma
Chronic negative pressure thins the TM and retracts, adhering to middle ear -> squamous epithelium forms inside and expands
|
Worsening hearing loss
Chronic discharge, fullness
Not painful
History of AOM or previous surgery
PE: pearly white mass, squamous debris, discharge
Conductive hearing loss
|  |
Necrotizing (Malignant) Otitis Externa
MC: diabetics, immunocompromised
MC pathogen: pseudomonas
|
Deep severe pain
Drainage, swollen red canal
Granulation tissue, osteomyelitis at skull-base, pain with talking/chewing
CN 7 and 12 involvement
TX: control DM, oral FQ
|  |
Mastoiditis
MC pathogen: S. pneumo, S. aureus
|
Fever, malaise, hearing loss, +/- headache
History of ABX use without improvement
PE: swollen over mastoid, redness, tenderness, LAD, outward protrusion of pinna
TX: IM ceftriaxone or IV ABX
CT Scan, refer to ENT
|  |
Labyrinthitis (otitis interna), vestibular neuronitis, vestibular neuritis
| ||
Etiology: viral, head injury, stress, allergy
|
Rapid onset severe vertigo (3-5 days), nausea, vomiting, imbalance
Preceding URTI
+/- nystagmus (severe)
|
Symptoms regress over 3-6 weeks
|
Central Vertigo
|
Peripheral Vertigo
|
Gradual and continuous symptoms, mild to moderate
Focal signs, nausea, vomiting, hearing loss (rare)
|
Acute and intermittent symptoms, but severe hearing loss, tinnitus, fullness
Hearing loss, severe nausea and vomiting, diaphoresis
|
Etiology: MS, brain tumor, head injury, medications
|
TX: Valium, Meclizine
|
- Acute otitis media - most common diagnosis for acute office visits in children
- Most common complication: tympanic membrane perforation
- Untreated complications - leads to facial nerve paralysis (Bell’s Palsy), cerebral venous sinus thrombosis, mastoiditis, short/long term hearing loss, speech delay, bacterial meningitis, intracranial abscess, TM perforation
- Bagel ear - bulging TM
- Most common cause of hearing loss: cerumen impaction
- Most common cause of unilateral sensory hearing loss: viral neuritis
- Presbycusis - Most common type of hearing loss in elderly
- Most common neuropathy associated with acoustic neuroma: loss of corneal reflex due to trigeminal involvement
- Bilateral nystagmus with cold caloric testing - signifies intact cortex, midbrain, and brainstem
- Recurrent unilateral serous otitis media - consider oropharyngeal cancer
- Drugs that cause nystagmus - MALES TIP
- Methanol
- Alcohol
- Lithium
- Ethylene glycol
- Sedative hypnotics, Solvents
- Thiamine depletion and Tegretol (carbamazepine)
- Isopropanol
- PCP, Phenytoin
- Medications that cause hearing loss: aminoglycosides, antineoplastic agents, loop diuretics, salicylates
- Meniere's Disease (endolymphatic hydrops) - excessive endolymph fluid in the cochlea overstimulates hairs causing vertigo and sudden hearing loss with aural fullness; most commonly unilateral and appears in adults
- SX: sudden vertigo, aural fullness or pressure, tinnitus, fluctuating hearing loss, nausea/vomiting, lasts hours
- TX: low salt, high water diet, diuretics, intratympanic steroids
- Avoid ETOH, caffeine, tobacco
- Dix-Hallpike Maneuver - diagnoses benign positional vertigo (eye twitching occurs), which is provoked by head movements or positioning
- Nystagmus - always positional, brief, and fatigable
- Rotatory nystagmus (posterior canal BPPV) - Epley maneuver
- Lateral nystagmus (lateral canal BPPV) - Lempert Maneuver
- Weber Test - sound is louder in ear with conductive loss
- Acoustic Neuroma (vestibular schwannoma) - tumor of 8th CN
- SX: unilateral hearing loss, vertigo (late), unsteadiness, tinnitus
- Bilateral acoustic neuroma - associated with Neurofibromatosis type II
- Decreased corneal sensitivity, diplopia, headache, facial weakness
- LP: elevated protein
- TX: MRI
- Eyes
- Myopia - “nearsighted”; vision rays come into focus in FRONT of retina
- Hyperopia - “Farsighted”; vision rays come into focus BEHIND retina
- Presbyopia - farsightedness caused by old age
- Strabismus (heterotropia) - eyes do not align (cross-eye)
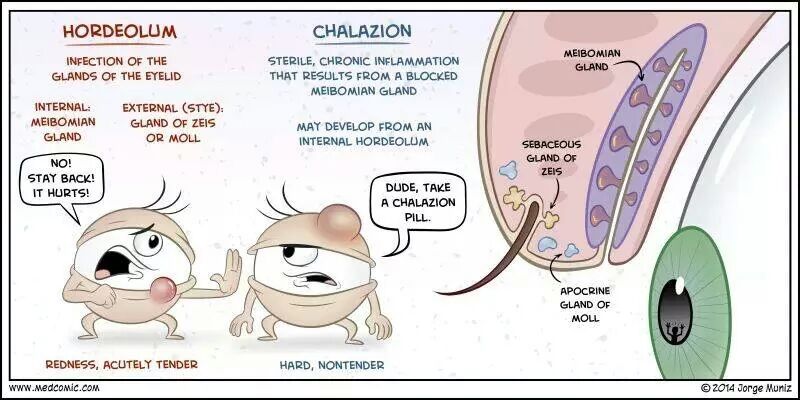
- Hordeolum - occurs on upper or lower eyelid; red and painful; spontaneously resolves
- Abscess of Meibomian gland (internal) - points toward conjunctiva
- Glands of Zeis (external, stye) infection at eyelid margin, pointing outward
- Chalazion - obstruction of meibomian gland (granuloma) or internal posterior hordeolum; painless, non-tender, non inflamed swelling (nodule) developing over the course of weeks (chronic)
- TX: hot compress, oral doxycycline or tetracycline
- Pterygium (Surfer’s Eye) - commonly grows from the nasal side of the conjunctiva
- Eyelid Malposition
- Retinoblastoma - child with blurry vision and abnormal pupillary reflex with a white reflex upon fundoscopic exam
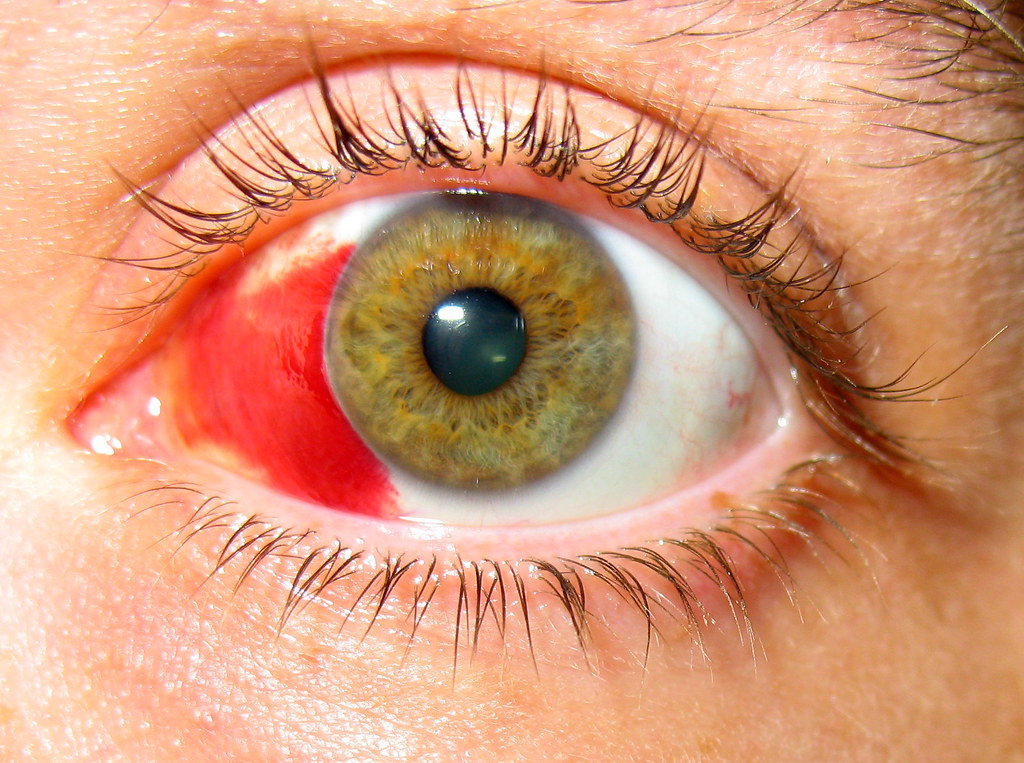
- Subconjunctival hemorrhage - bleeding of the conjunctival or episcleral blood vessels into the subconjunctival space; painless; self limiting - lasts 2 weeks
- Blepharitis - conjunctival and lid margin inflammation
- Slit lamp exam: greasy appearance of lid margin with scaling around the base of the lashes
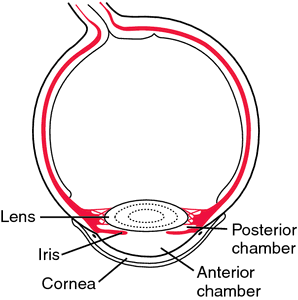
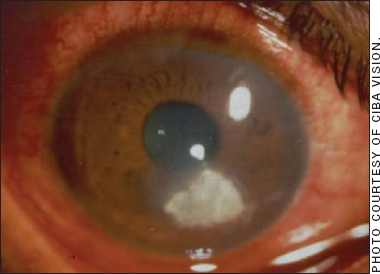
- Hypopyon - accumulation of white inflammatory exudate in the anterior chamber
- SX: painful, red eye
- Slit lamp exam: localized, white, flocculent infiltrate in anterior chamber
- Hyphema - blood in anterior chamber resulting from tears in ciliary body or iris root vessels; most common in children (70%)
- RF for rebleeding: sickle cell disease or trait, black, ASA use, prior low visual acuity, hyphema > ⅓ anterior chamber, treated after 24 hours, elevated IOP
- 4 S’s of Hyphema (Complications)
- Staining of the cornea
- Synechiae - iris adheres to cornea or lens
- Secondary rebleeds on 2-5th day (20%)
- Significantly increased IOP
- TX: Rest, elevation of head, topical steroids, avoid ASA/NSAID
- Welder’s Flash - severe eye pain and multiple pinpoint areas of fluorescein uptake representing ruptured corneal epithelial cells
- Slit lamp exam: Diffuse Punctate Keratopathy
- Most common pathogens of
- Chronic Dacryocystitis: candida albicans, anaerobic streptococci, staphylococcus epidermidis
- SX: painful erythema over the tear duct at nasal side of eye with small amount of pus draining from tear duct
- Dacryoadenitis - acute inflammation of the lacrimal gland seen in sterile inflammatory disease
- SX: abrupt onset swelling of upper eyelids, laterally;
- Most due to gram positive bacteria, but EBV most common virus
- Normal range of intraocular pressure (IOP): 10-23 mmHg
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
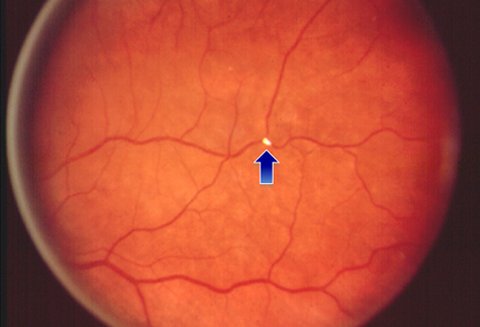
Central Retinal Artery Occlusion (cherry red spot, ischemic retina): flow through CRA occluded
Associated: atherosclerotic thrombosis, embolus, giant cell arteritis
SX: sudden painless loss of vision in one eye (unilateral)
PE: pale-gray retina, APD, cherry dot
Irreversible damage to retina after 90 minutes - IMMEDIATE CONSULT (decrease IOP & arterial dilation)
|  |
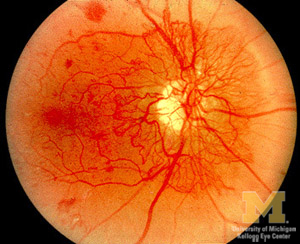
Central Retinal Vein Occlusion (Blood & Thunder Fundus): sudden, painless unilateral vision loss, 50+
PE: macular edema, cotton wool spot, massive superficial/deep hemorrhage with vitreous involvement
MC Associated: HTN, POAG
|  |
Age Related Macular Degeneration (ARMD): loss of central vision clarity, long smoking history, metabolic syndrome, FH, female, white, age 50+
PE: drusen formations, retinal atrophy
TX: Anti-VEGF intravitreal injections
|  |
Dry AMD (Nonexudative)
|
Wet AMD (Exudative)
|
Buildup of drusen
Mild - asymptomatic
Moderate - some vision loss
Severe - central blind spots
TX: vitamins to slow process
|
Choroidal neovascularization
Early - mild distortion
Late - central blind spot
|
{kind=link}
Differential of Red Eye with Decreased Visual Acuity
| |
|
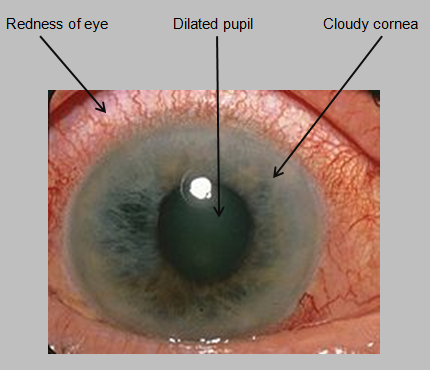
EMERGENT OPHTHALMOLOGY CONSULT
“Halos around lights” (bilateral)
Dull or severe pain, blurry vision, frontal headache, lacrimation, +/- nausea and vomiting
Pain more severe in dark
RF: asians, eskimos, hyperopes, elderly
IOP: 40-80 mmHg (sudden increase)
TX: IV mannitol, pilocarpine, IV acetazolamide, iridectomy
|  |
|
Visual changes begin peripherally
Gradual, painless loss of vision
More common than acute
4% of patients 40+
Most common cause: outflow obstruction through trabecular meshwork
| 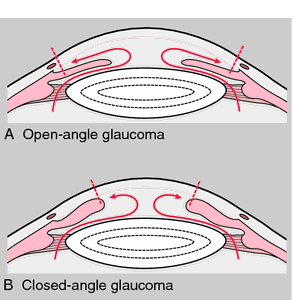 |
|
SX: eye/periorbital pain, consensual photophobia, hypopyon, irregular pupil,
Floaters, headaches, dilated ciliary vessels (ciliary injection or flush), “cells and flare” in anterior chamber, keratic precipitates (KP) on posterior surface of cornea
TX: refer to ophthalmology +/- rheumatology, steroid and dilating drops
|  |
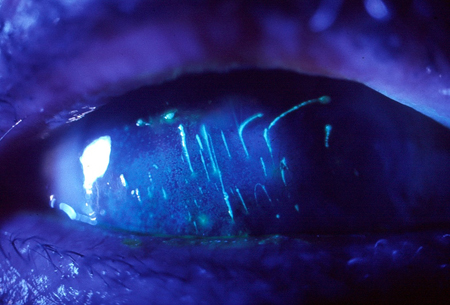
Corneal Abrasion
Multiple vertical linear abrasions (ice rink sign) under upper eyelid suggests foreign body
MC etiology: contact lenses
TX: cycloplegic, topical NSAID, topical antibiotic, oral analgesics/sedatives
Contraindicated: topical steroids, patching
|  |
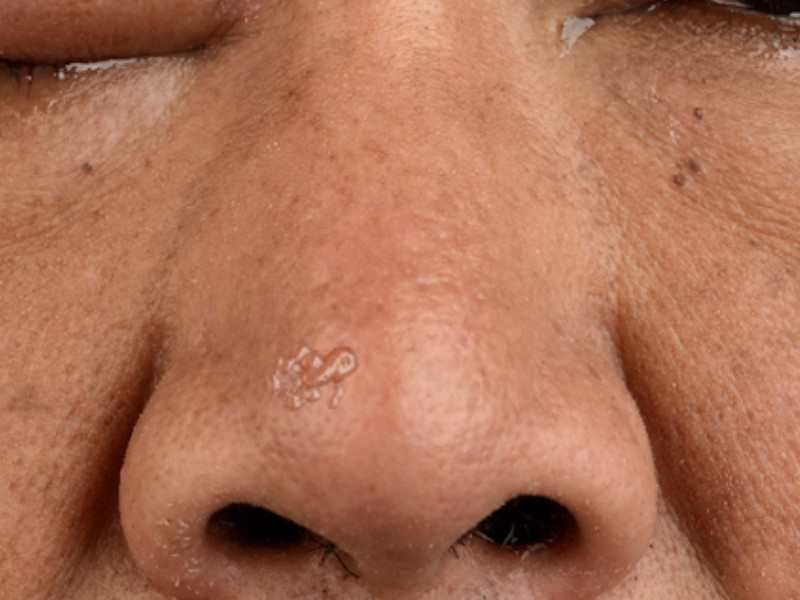
Herpes Simplex (HSV) Keratitis
EMERGENT OPHTHALMOLOGY CONSULT
Etiology: HSV-1
SX: painful eye, blurred vision, conjunctivitis, photophobia, tearing
Slit lamp exam: dendritic ulcer (branch-like) lesion
Hutchinson’s sign: herpetic lesion on tip of nose (nose and cornea supplied by nasociliary nerve)
TX: most spont. resolve in 3 weeks
Contraindicated: topical steroids or patching
|  |
Bacterial (Microbial) Keratitis
SX: rapid onset red, painful eye with discrete corneal infiltrate, photophobia, and decreased vision +/- hypopyon
(+) Seidel sign/test
Most common: pseudomonas (contact lens wearers), Enterobacter
VISION THREATENING PROCESS - rapid progression (24-48 h), REFER
If small, peripheral - FQ every 1-2 h
|  |
Conjunctival Injection
Anterior vessels - produce more redness, move with conjunctiva and constrict with vasoconstrictors
Posterior - stationary and less red
|  |
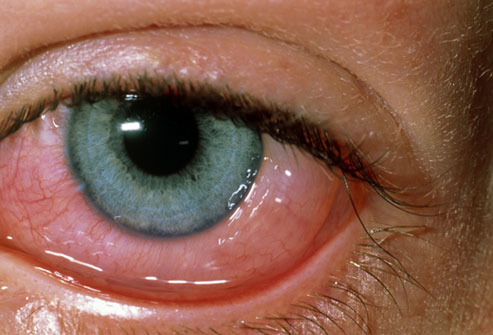
Viral Conjunctivitis (pink eye)
Most common: adenovirus
Associated symptoms: recent URTI, no resolution with eye drops
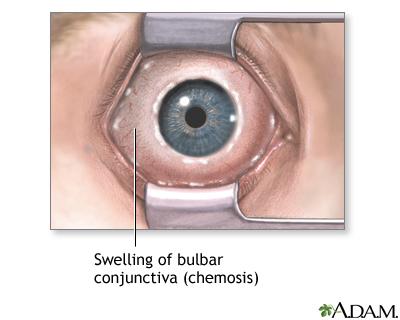
SX: unilateral or bilateral, benign, self-limiting (2-4 weeks), preauricular adenopathy, epiphora, hyperemia, chemosis, follicular conjunctival injection, subconjunctival hemorrhage
TX: supportive (cold compress, lubricants - artificial tears), hand hygiene
|  |
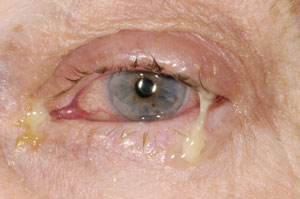
Bacterial Conjunctivitis
Associated: steroid or OTC eye drops, contact lens wearers, age, sexual activity, immunodeficiency
Segmental or diffuse injection, purulent discharge, “mattering” or lid margin, difficulty prying open lids after awakening
Topical FQ and erythromycin
|  |
|
SX: Itching, history of rhinitis, clear discharge, conjunctival injection +/- chemosis, +/- eyelid edema
Summer, Spring, Fall
Usually symptom free in winter
|  |
Vernal Keratoconjunctivitis (VKC)
Bilateral, chronic inflammation or “Spring catarrh” summer conjunctivitis
Shield ulcer (pathognomonic) caused by inflammatory mediator release
Onset in puberty
Most common in males
| 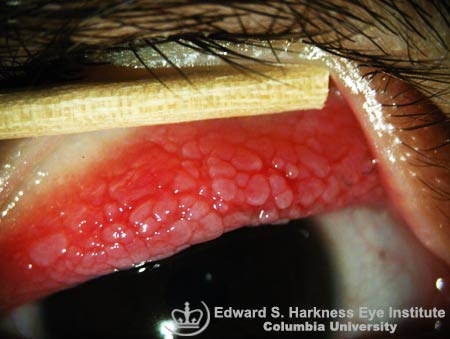 |
Giant Papillary Conjunctivitis (GPC)
RF: contact lens overuse, plastic prosthetic eye
First: itching with mucoid discharge
Large cobblestone papillae >0.3 mm
TX: stop wearing contact lenses
|  |
Atopic Keratoconjunctivitis (AKC)
Bilateral, inflammation of conjunctiva AND eyelids, eczematoid dermatitis of eyelid with dry, scaly, inflamed skin
Associated with atopic dermatitis (eczema)
TX: topical antihistamines, mast cell stabilizers, olopatadine, topical NSAID (ketorolac), topical steroid (prednisolone)
|  |
Gonococcal Conjunctivitis (neonatal = ophthalmia neonatorum)
N. gonorrhoeae or C. trachomatis
Pain, tenderness, hyperemia, chemosis
Purulent, mucoid or mucopurulent
May ulcerate, resulting in vision loss
|  |
Episcleritis: inflammation between conjunctiva and sclera (episcleral tissue)
Mild, self-limiting, recurrent
Vessels blanch with topical vasoconstrictors
2 Types
Simple: intermittent (1-3 months), lasts 7-10 days, mod-severe inflammation, spontaneously resolves after 2-3 weeks
Nodular (shown): prolonged, acute onset, mild-mod + systemic disease
TX: none required +/- oral NSAID
|  |
Scleritis: inflammation of the sclera
Diffuse or Nodular
VISION THREATENING - REFER IMMEDIATELY
SX: awakened from sleep due to deep boring pain, vessels will not blanch or move with topical vasoconstrictors
| |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
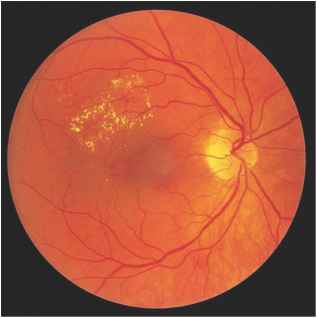
Hard Exudate: deep yellow with sharp margins; circinate
|
Leakage from pre-capillary arterioles
Ex. von Hippel Lindau disease, radiation, HTN
Most common cause: DM
|  |
|
Due to ischemia of superficial retina (microvasculature)
|
Neural micro infarctions
Ex. HIV, connective tissue disease, DM
Most common cause: HTN
Most common funduscopic exam finding in AIDS patients (CMV retinitis)
|  |
Retinal Drusen: clusters of yellow-orange spots, centered around fovea
|
Metabolic debris from retinal pigment epithelium
Most common cause: ARMD
|  |
Diabetic Proliferative Retinopathy
Prolonged hyperglycemia causes:
1. Basement membrane thickening
2. Decreased pericytes (hyperproliferation) 3. Microaneurysms 4. Neovascularization |
Neovascularization breaks through ILM (inner limiting membrane) leading to tractional retinal detachment
|  |
Non-proliferative Retinopathy
|
Aneurysms
Hard exudates Hemorrhage | 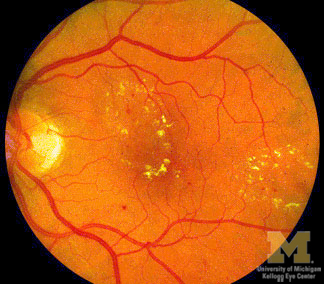 |
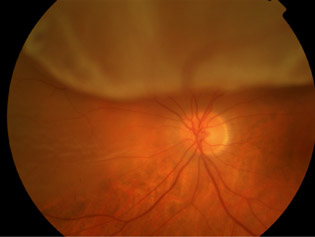
Papilledema: optic disc swelling caused by increased intracranial pressure (ICP)
|
Bilateral, develops over hours to weeks
Transient obscurations of vision (lasts seconds)
ICP: most commonly occurs bilaterally
|  |
Optic Neuritis: optic nerve swelling causes destruction of myelin sheath
Papillitis - head of optic nerve
Retrobulbar neuritis - posterior nerve
PAIN PRECEDES VISUAL LOSS
|
Most common cause: Multiple sclerosis
Normal ICP
Sudden unilateral loss of central vision
MC symptom: blurry or “foggy” vision
Pain with movement of affected eye (NOT RED)
PE: swollen disk, APD
TX: IV/oral steroids
|  |
Cataracts
Any opacity of the lens, whether visually significant or not
Most common cause: age related nuclear sclerosis
|
SX: glare, myopic shift, multiple images due to refraction, blurry vision
|  |
Retinal Hemorrhage
|
Causes: HTN, retinal vein occlusion, DM, shaken baby syndrome or severe head trauma
|  |
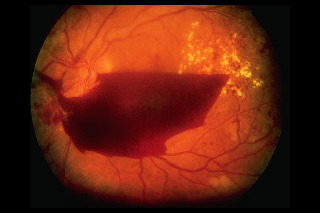
Vitreous Hemorrhage: extravasation (leakage) of blood into areas in and around vitreous humor
Age 50+
50-70% of acutely symptomatic patients have retinal detachment
|
Most common cause: proliferative diabetic retinopathy
Others: trauma, retinal detachment
“Flashing lights”, floaters
Blurry vision, reddish tint, photopsia (brief flashes of light in periphery)
Most asymptomatic
|  |
Retinal Detachment
EMERGENT OPHTHALMOLOGY CONSULT
Peripheral -> central vision loss
TX: inferior - patient sits up
superior - patient lies down
|
Preceded by posterior vitreous detachment: photopsia, floaters, feeling of heaviness in eye
Painless vision loss
“Curtain of darkness” with peripheral flashes or spider webs and floaters
Gray detached retina
|  |
Amaurosis Fugax
Etiology: atherosclerosis (retinal artery emboli), carotid stenosis
|
“Fleeting blindness” or “curtain coming down vertically into field of vision”
Painless, transient (quickly returns), unilateral visual loss
Lasts 2-20 minutes
|  |
Non-arteritic Anterior Ischemic Optic Neuropathy (NAION): damage to optic nerve head from microvascular occlusion
RF: HTN, DM, hypercholesterolemia, smoking
|
Sudden upon awakening, non-painful, unilateral optic disc swelling
Afferent pupillary defect (APD), most upper or lower half of visual field
Age: 50-70
Visual loss does not progress or recover
Resolves 4-8 weeks
| |
Arteritic Anterior Ischemic Optic Neuropathy (AION): damage to optic nerve head from microvascular occlusion
|
Age: 70-90 (older)
Severe visual loss, jaw claudication, temporal artery tenderness, temporal headache, unintentional weight loss, fatigue, myalgias, loss of appetite
Significant APD
DX: STAT ESR, temporal artery biopsy
TX: high dose steroids to prevent blindness in contralateral eye
| |
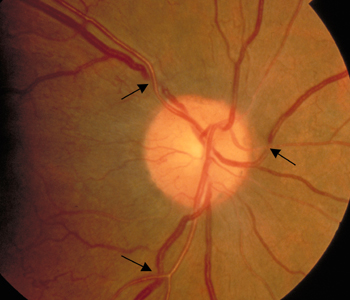
Hypertensive Retinopathy
|
Hallmark: Diffuse arteriolar narrowing (AV nicking)
|  |
Osteogenesis Imperfecta (brittle bone disease, Lobstein syndrome)
|
Blue-gray sclerae due to underlying choroidal veins showing through a thin sclera (defective Type 1 collagen)
Most common type of OI: Type 1
|  |
{kind=link}
{kind=link}
- Cellulitis
- Most common cause of orbital cellulitis: Staphylococcus aureus
- LIFE THREATENING - EMERGENT OPHTHALMOLOGY CONSULT
- Most common cause of periorbital (preseptal) and orbital infections: Staph aureus, Strep pneumo, and H. flu
Periorbital (preseptal) Cellulitis
| |
Gross lid edema, chemosis
Toxic, febrile
Proptosis, limitation of ocular mobility
+/- decreased vision
|
Lid edema, chemosis ONLY
NO proptosis, limitation of motility, or decreased vision
|
{kind=link}
{kind=link}
{kind=link}
- SX: decreased visual acuity, IOP (“Squishy eye”), bloody chemosis, visible wound of cornea/sclera, change in anterior chamber depth, displacement of pupil or shape, prolapse of ocular tissue (brown)
- Lateral canthotomy contraindicated if suspected ruptured globe!
- SX: Pain, eccyhmosis, bloody chemosis, resistance to retropulsion
- Afferent pupillary defect (APD)
- Increased IOP
- Most common pathogens causing bacterial conjunctivitis: Staph aureus, Strep pneumo, H. flu
- Most common cause of vision loss in patients 24-70 - Diabetic retinopathy
- Most common cause of vision loss in patients 65+ - Age related macular degeneration (ARMD)
- Most common cause of drusen - ARMD
- Most common cause of exudates: Diabetes
- Viral conjunctivitis - most commonly caused by Adenovirus
- Red-green color blindness - one of the most common genetic disorders, affecting 7% of all males
- Most common findings associated with orbital floor fractures: diplopia, globe lowering, numbness over the cheek (V2)
- Marcus Gunn Pupil (Afferent Pupillary Defect) - due to optic nerve damage or retinal detachment
- DX: Swinging Flashlight Test - decreased bilateral pupillary constriction when light shown in affected eye
- Most common conditions: ischemic optic neuropathy (ION), glaucoma, optic neuritis
- Seidel Test - assesses the presence of anterior chamber leakage in cornea, including post-trauma, corneal perforation or degeneration
- Tangential Light Test - determines the presence of narrow angle glaucoma or perforating corneal injury; if part of the iris is in the shadow, the angle is narrow
- Cycloplegics vs. Sympathomimetics
- Cycloplegics - inhibits parasympathetic stimulation which constricts the iris and inhibits the ciliary muscle, paralyzing the ciliary muscle and causing loss of accommodation (ex. atropine and cyclopentolate, scopolamine, tropicamide)
- Sympathomimetics - stimulates iris’ dilator muscle
{kind=link}
{kind=link}
Bilateral optic disk swelling
|
Unilateral optic disk swelling
|
Raised intracranial pressure, malignant hypertension
|
Optic neuritis, ION, central retinal vein occlusion, intracranial optic nerve compression, posterior scleritis
|
- Nose
Acute Viral Rhinosinusitis
(common cold, URI)
|
Influenza
|
Sinusitis
|
Etiology: adenovirus
Incubation: 2-4 d (3 day shed)
Direct contact, droplets
|
Influenza virus
Incubation: 1-4 d (infectious day before to 5 days after onset)
|
MC Etiology: antecedent viral URI, allergies, tumors, FB, deviated septum or polyps
MC sinus: maxillary (cheek pain), ethmoid (retro orbital pain), frontal (lower forehead)
MC pathogens: S. pneumo, H. flu, M. Cat
|
Const SX: Fever, chills, malaise
Rhinorrhea - clear, watery
Nasal congestion, sneezing
Sore throat, non-prod cough
Myalgia, headache
PE: low fever, nasal/throat erythema, congested turbinates/discharge, sinus tenderness, cervical LAD
|
Abrupt onset fever
Sore throat, retro-orbital headache, myalgias, malaise, nonproductive cough
PE: fever, clear nasal discharge, pharyngeal erythema, cervical LAD
|
Major Symptoms
Facial pressure or pain worse with bending forward
Nasal obstruction, discharge (purulent), hyposmia
Minor Symptoms
Fever, fatigue
Headache, halitosis, dental pain, cough, ear pressure
2 Major OR 2 Minor + 1 Major
PE: purulent discharge, PND, halitosis, sinus tenderness, transillumination of sinuses
|
Resolves 5-8 days
Analgesics: ASA, Tylenol, NSAIDs
Topical analgesics - Chloraseptic
Nasal saline washes, humidifier
Decongestants - Sudafed, Afrin
Mucolytic - Mucinex
Antihistamines - Benadryl, Claritin, Zyrtec, Allegra
|
Symptoms last 3 days to 2 weeks
Antipyretics, bedrest
Oseltamivir (Tamiflu) within 40 hours of symptom onset
IM/ID Vaccine for anyone >6 months up to 5 years and >50 years old
Nasal spray: non-preg 2-49
|
Acute: lasts <30 d with complete resolution
Subacute: 30-90 d with complete resolution
Chronic: >90 d with persistent symptoms
Non-contrast CT Scan - first line (chronic, unresponsive)
Sinus aspirate culture - gold standard
First line: Amoxicillin, Cefdinir (Omnicef) 10-14 d
Beyond 2 W: Augmentin, Cefuroxime
Chronic: add inhaled steroids
Severe: Levaquin, Bactrim
PCN Allergy: Azithro, Clarithro
|
Hydration, humidifiers, saline sprays
Decongestants: topical or PO
Analgesics: NSAID, Tylenol
If allergic: nasal steroids, antihistamines
Refer to ENT immediately: changes in vision, mentation, or periorbital edema
| ||
- Sinusitis - Maxillary most commonly affected, followed by ethmoid
- Most common etiology for acute sinusitis: antecedent viral URI
- Most common bacterial pathogens: strep. pneumo, H. flu, M. cat.
- Orbital Cellulitis - associated with ethmoid sinus
- SX: fever, eyelid edema, ptosis, proptosis, chemosis
- Osteomyelitis - Frontal sinus most commonly affected
- SX: fever, headache, doughy edema over bone, large forehead abscess
- Initially IgE mediated, then recruits neutrophils, eosinophils, lymphocytes
- SX:
- Irritative: sneezing, itching, rhinorrhea
- TX: antihistamines
- Congestive: congestion, stuffiness
- TX: decongestant (Sudafed, Afrin), anti-leukotriene
- First line: antihistamines, topical nasal steroids
- Adjunctive: mast cell stabilizer
- Vasomotor rhinitis - most common in anxious patients (non-allergic, unknown etiology), causes congestion & profuse rhinorrhea
- TX: topical anticholinergics (ipratropium bromide)
- Aspirin induced asthma (Samter's triad) - aspirin precipitates acute bronchospasm in patients with nasal polyps and asthma
- Triad: nasal polyps, asthma, Aspirin-sensitivity
- Nasal polyposis - usually bilateral; if unilateral, consider tumor; congestion & fullness
- Rhinitis medicamentosa - rebound rhinitis following sudden cessation of topical decongestants (3-5 d)
- SX: extreme nasal obstruction, pressure
- “3 sprays, 3 times daily, for 3 days”
- Squamous cell carcinoma - most common form of nasopharyngeal cancer
- Most common cause of Septal Hematoma: nasal trauma
- Saddle nose deformity - complication if untreated
- Toxic Shock Syndrome (TSS) - previous nasal packing for anterior nosebleed
- Etiology: toxin releasing S. aureus
- SX: fever, nausea, vomiting, and hypotension
- Most common cause of Epistaxis: digital trauma
- “Colder, older, males” - most commonly occurs in colder months, older population, and males
- Most common type of epistaxis: anterior epistaxis
{kind=link}
{kind=link}
{kind=link}
Anterior epistaxis
|
Posterior epistaxis
|
Origin: Kiesselbach plexus
Visualized easily
TX: anterior nasal pressure
|
Origin: sphenopalatine artery’s lateral nasal branch
Unable to visualize bleeding site, blood trickles down oropharynx and both sides of nose, unable to control with pressure
TX: posterior-anterior packing or balloon tamponade device
|
- Mouth/Throat
- Centor Criteria for diagnosis of Strep Throat - Fever > 38 C, lack of cough, tonsillar exudate, tender anterior cervical LAD (3 out of 4 present, sensitive)
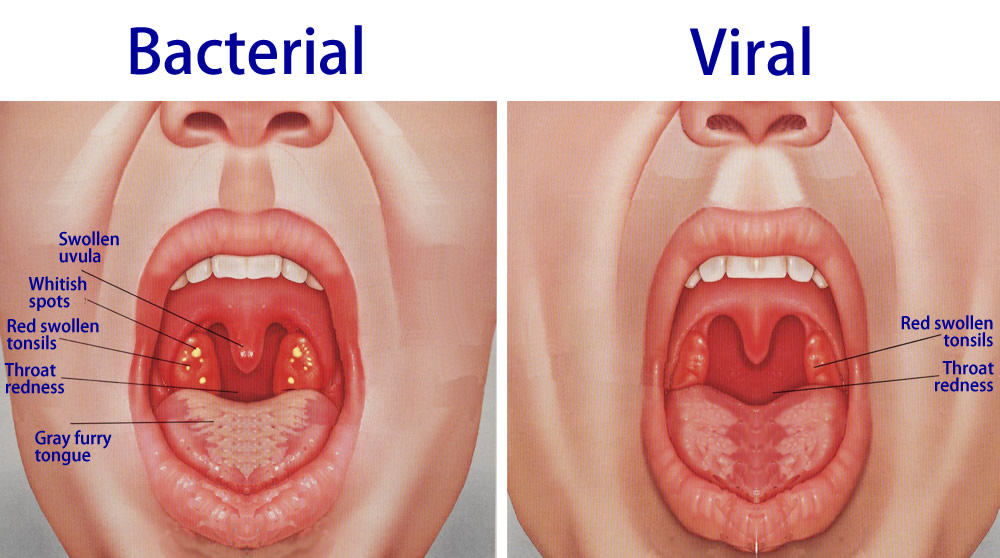
Etiology: Strep (GAS), Staph
Incubation: 12 h - 4 d
|
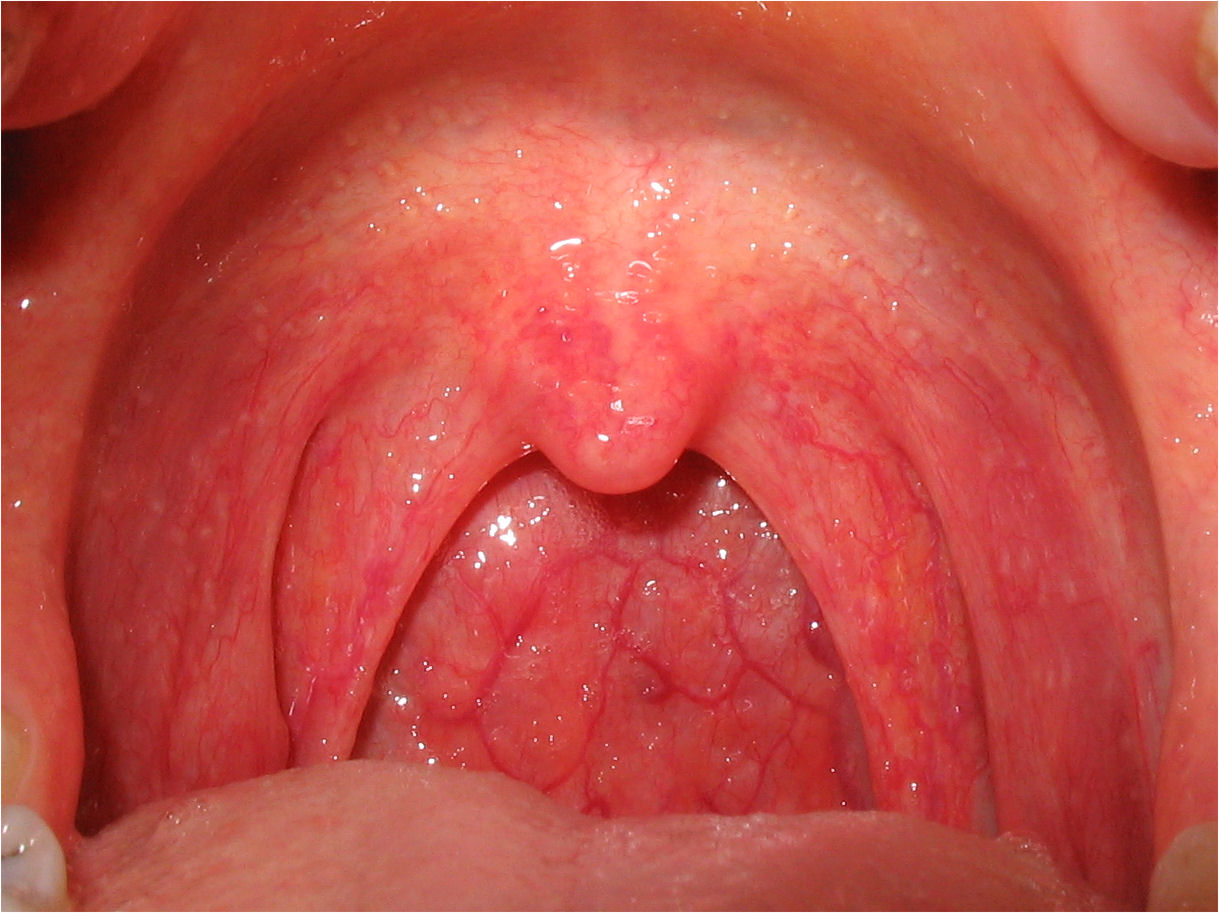
Etiology: Coxsackie A&B, adenovirus, rhinovirus, echovirus, HSV
|
EBV or CMV
Prodromal: 2-5 d (infectious)
|
SX > 1 week
Odynophagia, dysphagia, cough, hoarseness
Rhinorrhea
Fever, anterior cervical LAD (60%)
+/- Purulence
PE: tonsillar exudates
|
SX < 1 week
Odynophagia, dysphagia, cough, hoarseness
Rhinorrhea
LAD, myalgia, malaise, fever
|
Exudate - think EBV
Posterior cervical LAD
Splenomegaly, hepatomegaly
Sore throat
Fever, malaise
“hairy leukoplakia” - lateral tongue; will not scrape off
|
Rapid strep test (specific, less sensitive) - not required
|
CBC - lymphocytosis
Mono-spot test (specific, not sensitive), reveals previous infection
IgM & IgG titer to VCA, EA, EBNA (2-3 d for results)
| |
Hydration
1: Benzathine PCN, Pen-V K
2: Clinda, Amox, Cefuroxime
3: Levaquin, Cipro
Do not treat with Ampicillin: causes measles-like rash & type 3 immune-complex GN
|
Supportive: hydration, Tylenol
HSV: acyclovir
|
Supportive
Ampicillin
Avoid contact sports & being hit in abdomen
|
{kind=link}
{kind=link}
{kind=link}
Adolescents or adults
Incubation: 2-3 d
Drooling, sore throat, low fever, trismus (lock jaw), odynophagia
Ipsilateral otalgia
Unilateral swelling of soft palate, uvula deviation
Tonsillitis
|
IV hydration
IV Clindamycin or PCN
Intraoral drainage
Elective tonsillectomy
| ||
Retropharyngeal Abscess
|
Etiology: B-hemolytic Strep
Common 6 M to 3 y/o
Prefer supine position
Dysphagia, muffled voice, stridor, drooling
Fever, dyspnea, stiff neck
Cervical LAD
|
Lateral XR: wide retropharyngeal space at C4, air/fluid level
PE: Uvula/tonsil displaced away from abscess
|
ABCs
IV antibiotics
ICU admission
|
Corynebacterium diphtheriae (gram + rod) - exotoxins
MC: first decade of life
Sore throat, dysphagia, fever, tachycardia
Gray-black membrane - do NOT try to remove
|
Antitoxin (CDC)
| ||
N. gonorrhoeae
Asymptomatic or presents like bacterial/viral pharyngitis
Tonsillar hypertrophy
LAD
|
IM Ceftriaxone
Treat for Chlamydia - Azithromycin
| ||
MCC: Candida albicans
Cheesy, creamy mucosal plaques
|
Gram stain
Budding yeast with pseudohyphae
Can be scraped off
|
Oral Nystatin (swish & swallow)
PO Fluconazole
| |
Oral Cancer
|
Age: 50-60 with PMH of ETOH or smoking
SX: weight loss, localized pain
Odynophagia, dysphagia, oral mass, LAD, CN involvement
|
Refer
| |
Parotitis
|
Non-suppurative: paramyxovirus (mumps), influenza A, Coxsackie A, CMV, echovirus, Sjogren’s
Suppurative: Staph, strep
SX: Pain, swelling, pus from Stensen's duct (parotid)
|
CT
|
1. Clindamycin
2. Cefuroxime, Amox Hydration, warm compress, lemon drops |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
- Infectious Mononucleosis (EBV, CMV) - infects B-lymphocytes
- First line treatment for Group A beta-hemolytic strep: PCN
- PCN Allergy: Clindamycin or Erythromycin
- Most common sequelae: post-strep GN, rheumatic heart disease
- Dental abscess treatment - Clindamycin or Augmentin
- Dental caries - most common chronic disease in children
- Most common cause of xerostomia: medications (antihistamines and antidepressants)
- Most common form of glossitis: vitamin B12 deficiency
- Nutritional deficiencies leading to aphthous ulcers: B12, Folate, Iron
- Sialadenitis - most commonly affects the submandibular gland due to stasis of flow of saliva
- Infectious (children, post-op) - most commonly S. aureus, Strep pneumo, E. coli, H. flu
- Obstructive (more common form) - most common in middle-aged men
- Sialolithiasis (mealtime syndrome) - pain and swelling of submandibular gland worse with thought, smell, sight or taste of food
- Ludwig’s Angina - abscess of the submandibular, submental, or sublingual space
- Most common origin: lower second and third molar
- Most common agents: hemolytic strep, staph, mixed anaerobic/aerobic bacteria
- Alveolar osteitis (dry socket) - severe pain, foul mouth odor, and taste several days after tooth extraction
- Most common site affected in oral cancer: lateral ventral tongue
- Oropharyngeal thrush - most common oral manifestation of AIDS
- Epiglottitis - most common in 2-4 year old boys
- Viral pharyngitis - most common cause of pharyngitis
- Most commonly caused by Coxsackie A & B
- Most common viral agents of laryngotracheitis - parainfluenza virus I, II, III
- Most common bacterial agents: S. aureus, Strep. pneumo
- Herpangina - caused by Coxsackievirus group A
- Sjogren syndrome - most common in women 50+
- SX: diminished lacrimal and salivary gland secretion (dry mouth and eyes), salivary gland enlargement, arthritis
- Etiology: lymphatic infiltration of lacrimal/salivary glands
MC: 2-4 y/o boys
Etiology: HIB (children)
Child: fever, irritable, dysphonia, dysphagia
Drooling, inspiratory stridor
Adults: recent viral URI, severe pain, dysphagia, drooling, muffled voice
|
Clinical DX
High WBC, neutrophils
Lateral view: “Thumb print sign”
|
ABCs
ABX: 3rd Gen Cephalosporin, Unasyn
| |
Etiology: M. Cat, H. flu, N. gonorrhoeae
Non-infectious: reflux
Sudden onset hoarseness, rhinorrhea, cough, sore throat
|
Self-limiting: 2 weeks
Voice rest, hydration
Cough suppression - no antihistamines
| ||
Chronic Laryngitis
|
> 2 weeks
|
Refer
|
{kind=link}
{kind=link}
I'm surprised to see anything to do with eyes on the PANCE, I thought PAs weren't qualified to work for that specialty. Seeing as how I'm pre-PA and have been working with an ophthalmologist, do you happen to know if you ever see PAs working in that specialty?
ReplyDeletePAs are expected to do ophthalmic exams in any setting if any eye problems arise and know when there is an abnormality to refer. They can treat for simple things, like conjunctivitis, but like general physicians, they must know their limitations and know when they should refer to ophthalmologists. There aren't many PAs working in the ophthalmology field, but they are out there.
Delete^^^ The person above is exactly correct. We aren't expected to know everything as PAs. Just like other family physicians we have to know our limits and know when to refer, but we should have a basic understanding to know and recognize the signs/symptoms of emergencies.
DeleteHey Paul, the info in your website is wonderful!!!
ReplyDeleteOne quick question need your advise..
I read your previous article saying.. you do recommend the book of "The Color Atlas of Family Medicine" for family rotation.. now it has app (2013) about 94 bucks.. but the same company makes another app for another book of "The Atlas of Emergency Medicine" (2015) about 200 bucks..... I am new and currently doing family rotation right now, but will do ER later... do you recommend to buy both? or do you think I can buy ER one, do you think it can apply to family practice setting currently i am doing right now??? or ??? what you think? they are expensive.. I did research, but not useful results.. If possible, can you give me some advise plz, thank you very much in advance!!!
Pauline
I would probably read reviews on each and make that decision yourself. I'd hate to recommend one and it not be quality. If you plan on keeping it and using it for a long time, I would probably invest in the higher paying one if it is worth the money. Again, read reviews on each and decide whether you think the other is worth the extra $100. I would not recommend buying both, though.
DeleteThank you very much for your inputs!!!
DeleteHey Paul! Great site! Would you be able to upload these study guys as a pdf or word doc so that i can download it? This site is super informative!
ReplyDeleteHi GatorACE - great question! I'm actually working to format these into study guides for students. Give me a few more months and I should have everything worked out! Thanks for the motivation!
DeleteHi Paul ! This is awesome, any updates on being able to save it as a PDF? Maybe I just can't find it? Would love to have it for my subway commute
DeleteHey Christine,
DeleteGreat question! I have not released these as PDFs because I do not own the copyrights to the images.